

Digestive and gut issues
As a society, we are living in ways that don’t always support our optimum health, and this is particularly true when it comes to how we are digesting (or not digesting, as the case may be) our food.
There are a number of root causes of digestive issues that we can relate to our Western lifestyle, and, if these are left unchecked, can result in physical illness and discomfort. Because of our current medical model – which treats symptoms rather than addresses underlying issues – many of the people I see in my clinic with gut and digestive issues have been suffering for a very long time.
The good news is that the Functional Medicine approach has much to offer – in terms of both hope and interventions – for anyone looking to restore and support digestive health.
Many of us can relate to the idea of eating on the go, or reaching for high carb/high sugar snacks in the petrol station as we head off for another busy day. Eating at our desk while we pile through emails and return calls is not alien to us.
And, even if we do eat at home, the foods we are preparing often have an element of convenience – whether they are microwave meals, frozen produce, or take outs.
Our fast-paced lives simply don’t afford the same time to shop for, prepare and enjoy our meals. All of which aid good digestion. I have written more extensively about this topic in a recent blog post titled ‘Why digestion starts with the senses’. You can click here to read the article in full.
In short, however, it’s fair to say that there are a multitude of physiological processes that need to work in harmony in order to aid good digestion.
Many people who have digestive disorders do not always experience obvious symptoms and, in some case, will experience no symptoms whatsoever.
Having said that, health issues associated with digestion and the gut can present in a number of ways, and here I have provided more information about the different issues together with associated symptoms.
Click on the tabs below to read more:
Irritable Bowel Syndrome (IBS)
IBS is one of the more common digestive issues, however, it is more complicated than constipation or diarrhoea. IBS affects all members of the population but is more commonly found in women, with an average age of onset between 20 and 40 years old. Up to 1 in 8 people experience symptoms at any particular given time.
There are several subtypes of IBS, based on the predominant symptoms:
- IBS-C with constipation
- IBS -D with diarrhoea
- IBS-M mix of constipation and diarrhea
- IBS-U Unclassified – Bowel habits cannot be accurately categorized into one of the subtypes above.
Although the exact cause of IBS is currently unknown, Functional GI Disorders describe a group of conditions for which no structural cause has been identified. They occur as a result of disorder of gut-brain communications, and IBS is thought to be a multifaceted disorder involving changes in gastrointestinal motility (the movement of food through the GI tract), heightened pain sensations within the internal organs (hypersensitivity of gastrointestinal nerves), carbohydrate or bile acid malabsorption, emotional stress, gut bacteria imbalance that in turn affects the enteric nervous system, immune system, mucosal barrier and function, the balance of neurotransmitters, the balance of hormones and emotional wellbeing.
IBS and the multifaceted approach. Figure below explains the core and wider-ranging effects.
Somatic Symptom Disorder
Image: www.semanticscholar.org
Symptoms
IBS is characterized by abdominal pain or discomfort that may be associated with an alteration in bowel habits or defecation. Changes in bowel habits can include:
Diarrhoea
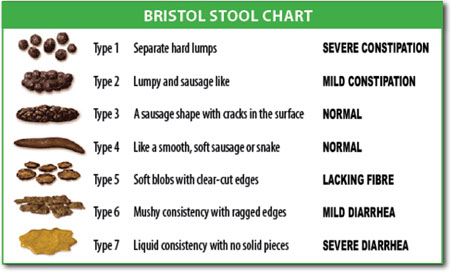
Diarrhoea is defined as loose or watery stools for more than 25% of the time, for a minimum of 3 months. This rapid transit is indicated on The Bristol Stool Chart as types 6/7. This is a common problem, and it is estimated that up to 70% of IBS sufferers experience chronic diarrhea, with half of them experiencing diarrhea most of the time. The other half is said to alternate between diarrhea and constipation. Diarrhoea can have a huge impact on quality of life and can be extremely stressful. What’s more, stress and anxiety can decrease transit time through the gut, therefore resulting in diarrhea, due to the influence on your digestive system by your nervous system. This can lead to a vicious circle of symptoms: diarrhea, resulting in stress, that can cause diarrhea.
Constipation
Constipation is extremely common, and yet one of the issues we face is in actually defining what constipation is. One of the most common explanations amongst medical professionals is actually constipation is less than Three bowel movements per week. However, most individuals have a differing opinion and as this is such an individual symptom, asking 100 people may produce 100 different answers. When surveyed, 98% reported that they experience between three bowel movements per day and three bowel movements per week. Ideally, we should be emptying our bowels on a daily basis.
On the Bristol Stool Chart below:
Types 1 and 2 (hard lumpy stools) are regarded as a sign of constipation and are usually accompanied by straining, difficulty and discomfort.
Normal transit time varies between 30 – 40 hours. Transit time in IBS can vary between 7 hours (diarrhea) and 96 hours (constipation).
If your transit time is slow (as in constipation), the stool can remain in your colon and become drier as you reabsorb the water it contains – hence the compact shape.
Types 3 and 4 on the chart are the ideal stools, which should be soft and easy to pass.
Bloating
Bloating occurs when your abdomen feels swollen, distended, windy, full, tight or hard.
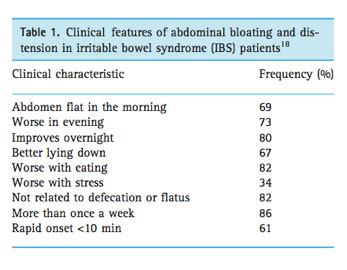
Bloating and distension can be caused by different mechanisms. Distension can result from fermentation of fibres by the bacteria in your gut, which can increase gas and therefore swelling. If you are more sensitive and/or feel bloated after eating, this may be the result of the normal pressure of food on the gut wall, which you feel more intensively with IBS. Clinical features of abdominal bloating and distension in IBS are listed in the table below:
Pain
Abdominal Pain is a classic feature of IBS and can occur daily, but commonly is present for approximately 3 days per week. IBS-related pain has certain features including:
- Can be related to changes in stool habits – such as diarrhea and constipation;
- At times, is relieved by bowel movements;
- Often tenderness in the left lower area of the abdomen is present;
- Often worse after eating.
IBS sufferers tend to be more sensitive in the gut, so may experience pain and discomfort from the normal passage of food or gas. This can result in persistent chronic pain with systemic effects.
Pain signals are communicated through sensory nerve cells in the gut, via the spinal cord, to the brain. If this continually occurs, pain signaling can actually alter your response to how you process pain and the influences of pain perception (throughout the body) which can result in chronic hypersensitivity, meaning that things that should not be painful, actually result in pain (like the passage of food in your gut).Other IBS symptoms include: early satiety, incomplete evacuation of bowels, nausea, indigestion (dyspepsia), swallowing difficulties (dysphagia) and reflux.
Systemic Symptoms
IBS is also associated with symptoms beyond the gut. These include
- Fatigue
- Backache
- Headaches
- Nausea and/or vomiting
- Urinary issues
- Difficulty swallowing
- Unpleasant taste in the mouth
IBS symptoms can happily overlap with other conditions, potentially revealing that differing disease symptoms may be the result of the same underlying causes. There are also diseases/condition that are more common in those with IBS. These include:
- Chronic fatigue syndrome
- Fibromyalgia
- Depression
- Anxiety, GORD (Gastro-oesophageal reflux disease)
- Gastritis (functional dyspepsia)
- Chronic Pelvic Pain Syndrome
- Tempromandibular joint disorder
Underlying causes of IBS
Functional Disturbances in the following area’s may all feed into Irritable Bowel Syndrome:
Underlying Causes:
image by: www.mdpi.com
Some of the most common reasons I see in my clinic include:
Visceral Hypersensitivity. Heightened gut sensitivity. This may be due to inflammation caused by infection, stress or diet but can remain even if these triggers are removed;
Dysbiosis. Bacterial imbalance in the gut. This can also lead to abnormal levels of serotonin in the gut;
Inflammation. Low grade inflammation is believed to be crucially implicated in the development of IBS, leading to alterations in gut permeability (leaky gut), hypersensitivity of gastrointestinal nerves and alterations in the processing of serotonin.
Intestinal Permeability. For more information about this, you can click here.
Stress. Anxiety and stress frequently present in clients with IBS and can actually arise from gastrointestinal upset. You can read more about stress in my blog post here;
Celiac Disease. Please click here for more information;
Poor Diet. Deficiencies in essential vitamins, minerals and fats and ingestion of certain foods, including gluten, lactose and a predominantly western diet that is high in sugars and carbohydrates may all contribute as dietary triggers to the development of IBS;
Small Intestine Bacterial Overgrowth. Parasitic Infection, dysbiosis (imbalance in your gut bacteria), inflammation, yeast overgrowth and the efficiency of digestion and absorption and gut immune function can all be assessed via functional testing.
Nutritional Considerations:
The functional approach to IBS involves identifying the underlying causes of the condition and addressing imbalances in digestive function and the lifestyle influences that may be triggering or contributing to the condition.
The following video from leading functional medicine doctor Dr Mark Hyman discusses the root causes and solutions to IBS:


Inflammatory Bowel Disease (IBD)
Inflammatory Bowel Disease is a term that refers to conditions of chronic inflammation of the gastrointestinal tract. This video provides a useful overview of the topic. Within the human body, the gastrointestinal tract contains the greatest density of commensal organisms which provides an unprecedented cluster of immune regulating functions which inhibit excessive responses from the immune system against harmless or non-dangerous antigens (toxins/foreign substances etc), including those asserted by the microbiome. Disruptions to these governing regulatory mechanisms results in a group of chronic inflammatory diseases that, collectively are referred to as Inflammatory Bowel Disease (IBD). Crohn’s disease (CD) and Ulcerative Colitis (UC) are the most well-known of the conditions that both fall under the IBD umbrella. These conditions are classed as autoimmune conditions as they are caused by an abnormal immune system response that results in your own immune system attacking your body’s healthy tissues. Both conditions are chronic and relapsing and are characterised by: Abdominal PainDiarrhoeaBloody StoolsAnd can also induce fatigue, fever, poor appetite and weight loss Other less common IBD conditions include: Microscopic colitisBehcet’s DiseaseLymphocyte colitisCollagenous colitisDiverticulosis-associated colitis UC and CD both share some similarities in their pathology and symptoms, but there are, however, differences in these two conditions: Ulcerative colitis: affects only the mucosal layer of the rectum or large intestine – or colon. When this becomes inflamed, it is referred to as colitis. This may be acute or chronic (long lasting), but the damage generally affects the entire colon and causes ulcers (sores) in the innermost layer of the colon. Crohn’s disease can affect any part of the digestive tract either in isolation or at multiple sites, with the damage generally occurring in patches as opposed to the entire tract. Several deeper layers of tissue within the intestines may be affected and may cause complications including abscesses, fistulas and strictures. CausesRecent research indicates four main areas of influence in the development of Inflammatory Bowel Disease: Genetic SusceptibilityExternal EnvironmentThe Intestinal MicrobiomeImmune Response Genetics Recent advances in genetic testing have implicated 163 genes that are associated with IBD, some associated with both conditions, others specific to the separate diseases. However, research & studies have found that although the genetic influences are critical in the development of IBD, they only account for 20-25% of the heritability of the conditions. However, both crohn’s disease (CD) and ulcerative colitis (UC) are associated with genes that are crucial to the preservation of the gut barrier and the subsequent response of the immune system. Environment There are many environmental factors that are thought of as risk factors for IBD. These include: SmokingDietDrugsGeographySocial StressPsychological influence Microbiome Our gut is densely inhabited by approximately 10 ¹4 microorganisms that live in harmony with us, their host. The bacteria have many beneficial roles including that of protection against pathogenic bacteria, they make certain vitamins, they enforce barrier function of the gut and support immunity which also includes limiting inflammation. Currently, we are able to culture approximately 20%-30% of the gut microbiome, but within this range there has been an association established between changes in the microbiome and IBD. Numerous studies have demonstrated a significantly reduced diversity of bacteria in IBD cases, irrespective of whether there was current inflammation or not. It has also been observed that the microbiome of IBD patients is unstable – compared to healthy individuals, with inadequate levels of key strains of bacteria and increases in opportunistic and pathogenic bacteria. Significantly, crohn’s disease is associated with bacteria that are fundamentally inflammatory so ‘blur the line’ between friendly and pathogenic (disease-producing) organisms. Immune factors The immune system can be looked at as an organ that is located throughout the body to defend you against pathogens wherever they invade or circulate. There are a set of distinctly different sections that are designed to respond appropriately to an invader in specific parts of the body. Mucosal Immunity describes the compartment that is located near to surfaces where most invasions occur and includes the gut, which acts as a gateway to an ever-increasing amount of foreign substances (antigens) in our food. The immune system has developed techniques to prevent excessive immune responses to food antigens whilst also maintaining the balance of detecting and killing pathogenic organisms entering via the gut. Despite the many regulating mechanisms, numerous pathogens can seep through the gut barrier and play a role in the development of IBD, if they are not eradicated by the immune system. In healthy individuals, pathogens are controlled by beneficial bacteria and harmony is maintained.In IBD, the combination of genetic influence and environmental factors (which include smoking, diet, lifestyle, major life stressors, medication use, air pollution, infections etc) can lead to dysbiosis (microbial imbalance). This disturbs the integrity of the gut barrier and influences the immune system resulting in rampant chronic inflammation and the subsequent changes in immune function. In summary, this inappropriate intestinal immune response to intestinal bacteria causes a chronic inflammatory condition, resulting in IBD. Nutritional & Functional Medicine Therapeutic recommendations: We are all unique and functional medicine works by personalising support to your specific situation. There is no one size fits all, your own diet, lifestyle, condition and current symptoms will dictate your needs. Addressing IBD is a step by step process that involves rebalancing the immune system, reducing inflammation and supporting tissue repair, supporting the gut and microbiome, supporting sleep, addressing nutritional deficiencies and reducing & removing environmental triggers. However, one of the most important areas to address is diet and specifically nutrient deficiencies that may arise from the reduction of nutrient absorption. Malnutrition is a major component of IBD with an estimated 65-75% of CD patients and 18-62% of UC patients effected. Diet and functional foods can imprint a significant influence in IBD and by excluding foods that may produce an inflammatory response, symptoms may be reduced.Adding foods that can reduce inflammation can be extremely supportive and you need to undertake both these measures in conjunction with each other. A Diet high in fibre has been found to reduce the risk of CD by 40% yet exposure to a diet rich in saturated fatty acids and processed meats has been reported to increase the risk of IBD. https://www.mdpi.com/2072-6643/9/3/259/htm Figure 1 Features of nutritional and functional medicine support Studies show: Treatment of patients with mild to moderate UC, not responding to conventional therapy, with a specific combination of probiotic therapy, resulted in a remission/response rate of 77% with no adverse effects. Dietary fibres, probiotics, non-starch polysaccharides & fat-soluble vitamins have been effective in ameliorating gastrointestinal inflammation. Functional foods have exhibited strong anti-inflammatory effects against IBD and can interact with the immune system to produce anti-inflammatory effects against IBD. Vitamin D deficiency is common in IBD patients with a frequency ranging from 16% to 95%. Vitamin D deficiency may also influence the severity of inflammation in IBD. Stress reduction is associated with decreased relapse in patients with CD or UC. Studies show that curcumin at a dose of 2g/day, when added to standard therapy, significantly reduced relapse rates in UC.
These include Inflammatory Bowel Disease, and other auto immune-diseases that manifest in the gut:
- Crohn’s disease (CD)
- Ulcerative Colitis
For further information about autoimmune disease, please visit this link.
If you think you are suffering from IBS or any of the IDB disorders and are looking for information on how to overcome it, please get in touch to find out more.
References
Al Mijan, M. Ou Lim, B. Diets, Functional Foods and Neutraceuticals as alternative therapies for inflammatory bowel disease: Present status and future trends, World J Gastroenterol, 2018; 24 (5): pp.2673-2685.
Belkaid, Y. Hand, T. Role of the Microbiota in Immunity and Inflammation, Cell, 2014; 157 (1): p.121-141.
Small Intestine Bacterial Overgrowth (SIBO)
SIBO is characterised by the presence of an abnormally high number and/or type of bacteria present in the small intestine. The small bowel is approximately 20 feet long and normally houses a small number of differing bacteria in comparison to the large bowel.
The small bowel is where we absorb nutrients, where certain bacteria produce nutrients including short chain fatty acids and vitamins including B Vitamins and vitamin K. The small bowel/intestine also houses a crucial proportion of the immune system that provides protection against invading microbes and it also helps neutralize pathogenic (bad) bacteria.
SIBO can affect the digestion and absorption of nutrients potentially resulting in nutritional deficiencies and increased risk of intestinal permeability (or leaky gut) which can ultimately result in increased immune reactions leading to food sensitivities, allergies, inflammation and autoimmune diseases.
There are various reasons why you may have SIBO, however it is mostly found after surgery when we see an overgrowth of bacteria.
SIBO is less likely a result of lifestyle factors.
These additional bacteria found in SIBO typically ferment carbohydrates from the diet and are involved in the development of symptoms which include:
- Bloating
- Increased production of gas
- Belching
- Abdominal pain, discomfort and/or cramps
- Constipation, diarrhoea or a combination of both
- Heartburn
- Nausea
- Reduced absorption of nutrients
- Systemic symptoms including headache, joint/muscle pain, fatigue, and rosacea.
Underlying causes of SIBO
SIBO is due to a failure of 1 or more of the body’s protective mechanisms that prevent bacterial accumulation in the Small Intestine.
Primary Underlying causes:
Small Intestine Motility Deficiency
Anatomical alterations:
- Obstruction
- Blind loop
- Fistula from large intestine to small intestine
- Absent/dysfunctional ileocecal valve
Risk Factors:
- Immunodeficiency
- Low stomach acid (Hypochlorhydria)
- Deficient Bile
- Deficient Enzymes
- Irritable bowel syndrome
- Bowel surgery
- Diabetes
- Crohns disease
- Numerous courses of Antibiotics
Chronic conditions of the organs of the digestive system – liver, pancreatitis, kidneys.
SIBO can also be the result of food poisoning. This is an auto-immune condition known as Post-Infectious IBS (PI-IBS), which is thought to account for 2/3 of IBS cases.
However, not all SIBO is PI-IBS and not all SIBO is triggered by food poisoning.
Clinical manifestations of SIBO
SIBO breathe tests can determine the subtype of the condition and the type severity of gas or gases involved. SIBO can be addressed by a combination of diet & lifestyle alterations, herbal antibiotics and in severe cases may require antibiotics from your GP.
SIBO can be a stubborn condition to rebalance, especially as we are all individual and SIBO can vary from person to person. However dietary interventions can be very successful at improving symptoms whilst the underlying causes are investigated.
Functional Medicine Doctor Dr Maxine Barish discusses SIBO in the following short video:
If you think you are suffering from SIBO and are looking for information on how to overcome it, please get in touch to find out more.
References
References for IBS
Agrawal, A. Whorwell, P. (2007). Review Article: Abdominal Bloating and Distension in Functional Gastrointestinal Disorders – epidemiology and exploration of possible mechanisms, Aliment Pharmacol Ther,27 (1), 2-10.
Bouin, M. Plourde, V. Boivin, B. (2002). Rectal distension testing in patients with irritable bowel syndrome: Sensitivity, specificity, and predictive values of pain sensory thresholds, Gastroenterology, 122 (7): 1771-1777.
Brown, B. (2019). Does Irritable Bowel Syndrome Exist? Identifiable and Treatable causes of associated Symptoms Suggest it May Not, Gastrointest Disord; 1(3):314-340.
Creed, F. Lea, R. Whorwell, P. (2007). Is Visceral Hyposensitivity Associated with Abdominal Distension in Irritable Bowel Syndrome, Gut, 56 (Suppl.2): A62.
Drossman, D. (2016). Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV, Gastroenterology, 150 (6):1262-1279.e2.
Lacy, B. Mearin, F. Chang, L. (2016). Bowel Disorders, Gastroenterology, 150:1393-1407.
Lacy, B. Patel, N. (2017). Rome Criteria and a Diagnostic Approach to Irritable Bowel Syndrome, Journal of Clinical Medicine, Nov, 6 (11): 99.
Leung, R. Riutta, T. Kotecha, J. (2011). Chronic Constipation: An Evidence Based Review, J Am Board Fam Med, Jul-Aug;24 (4): 436-451.
Nicholl, B. Halder, S. Macfarlane, G. (2008). Psychosocial risk markers for new onset irritable bowel syndrome – results of a large prospective population-based study, Pain, Jun 30; 137 (1): 147-155.
Spiller, R. Aziz, Q. Creed, F. (2007). Clinical Services Committee of The British Society of Gastroenterology. Guidelines on the Irritable Bowel Syndrome: mechanisms and practical management. Gut, Dec;56 (12):1770-1798.
Staud, R. Rodriguez, M. (2006). Mechanisms of Disease: Pain in Fibromyalgia Syndrome. Nat Clin Pract Rheumatol, Feb;2 (2): 90-98.
Whorwell, P. McCallum, M. Creed, F. (1986). Non-Colonic Features of Irritable Bowel Syndrome, Gut, Jan;27 (1): 37-40.
References SIBO
Dukowicz, A. Lacy, B. Levine, G. (2007). Small Intestinal Bacterial Overgrowth: A Comprehensive Review, Gastroenterology & Hepatology; 3 (2): 112-122.
Fassano, A. (2012). Leaky Gut and Autoimmune Diseases, Clin Rev Allergy Immunol; 42 (1):71-78.
Morowitz, M. Carlisle, E. Alverdy, J. (2011). Contributions of Intestinal Bacteria to Nutrition and Metabolism in the Critically Ill, Surg Clin North Am, 31 (4): 771-785.
Santaolalla, R. Abrue, M. (2013). Innate Immunity in the Small Intestine, Curr Opin Gastroenterol; 28(2):124-129.
Shah, E. Riddle, M. Chang, C. (2012). Estimating the Contribution of Acute Gastroenteritis to the Overall Prevalence of Irritable Bowel Syndrome, JNM, 18 (2):200-204.
References Bloating
Agrawal, A. Whorwell, P. (2008). Review Artlice: Abdominal Bloating and Distension in Functional Gastrointestinal Disorders – Epidemiology and Exploration of Possible Mechanisms, Aliment Pharmacol Ther; 27, pp.2-10.



